BJC Flex
Coming out of the pandemic, it was no secret that nurses were overworked, understaffed, and burned out, resulting in high staff turnover and soaring nurse agency spend. As an attempt at finding areas that we could help reduce and alleviate this burnout, I conducted extensive discovery work with nurses, patient care techs, and nurse managers to identify what areas had potential for either process or technological solutions.

Overview
BJC Flex is a mobile web application designed and built in-house by BJC Healthcare, St. Louis’ largest hospital system. By replacing outdated technology, standardizing processes, and empowering staff to pick up shifts in flexible increments, we were able to reduce costly agency spend and increase overall nurse satisfaction.
My Role:
Product Designer - collaborated with Stakeholders and Product Team to ensure an intuitive and meaningful user experience. I crafted research plans, collected and synthesized feedback, laid out the site architecture, and designed the overall look and feel of BJC Flex while contributing to the overall design system of BJC Healthcare.
Timeline:
2.5 Years
Tools:
Figma
Jira
Miro
Microsoft Suite
Dovetail
Collaboration:
Stakeholders:
Cross-collaborative team involving hospital and nursing leadership, HR, and operations.
Product Team
1 Product Manager
1 UX Architect
1 UX Intern
1 Agile Coach
6 Developers
The Initial Scope: Nurse Shift Hand-Offs
When I first started at BJC, I was initially told to focus on nurse shift-handoffs, when incoming nurses talk with outgoing nurses about their patients, medications, tubes, and family dynamics at both the beginning and end of every shift. This has historically been a thorn in the sides of hospital administration due to:
Inefficiency
Hand-offs are time intensive, oftentimes taking 30-45 minutes at the beginning and end of each shift.
HIPA
Nurses write everything on paper, including confidential patient information, that is then at risk of being left behind.
Lack of Standardization
No hospital, floor, or even individual nurse handled their hand-offs the same way, creating confusion and difficulty for staff floating between units.
However, regular attempts at process changes typically ended with limited results. With the digital capabilities brought by my newly formed UX team, this was seen as a prime opportunity to try again.

Research
Secondary Research: In order to be as efficient and cost-effective as possible and ensure that we weren’t conducting redundant research I reviewed previous research endeavors at BJC Healthcare, trying to determine what was relevant to our goal of understanding nurses in general, and the nurse shift hand-off specifically. We also reviewed available material from academic and medical journals to see how other organizations had responded to similar concerns. However, we found much of the material available to be outdated and irrelevant, spurring us on to go more in depth with our own research that we had initially assumed would be needed.
Contextual Inquiries: I spent over 100 hours shadowing 48 different frontline nurses and patient care techs at BJH, Shiloh, and Missouri Baptist, covering what we believed to be the full spectrum of the BJC system in as efficient a manner as possible, going to urban, suburban, and rural hospitals with a range of patients and different need and socio-economic levels. We also shadowed at a diverse array of floors at those hospitals, covering units as varied as general medicine, orthopedics, and the trauma ICU, in order to better understand the full nurse experience instead of just gathering floor specific knowledge.
Interviews: Along with the above research, I also interviewed 20 nurses from 5 different hospitals, continuing to cast a broad net throughout the hospital system. I also interviewed a broad range of nurse types, including House Supervisors, Assistant Nurse Managers, Travel Nurses, Nurse Educators, and Floor Nurses.
Deliverables:
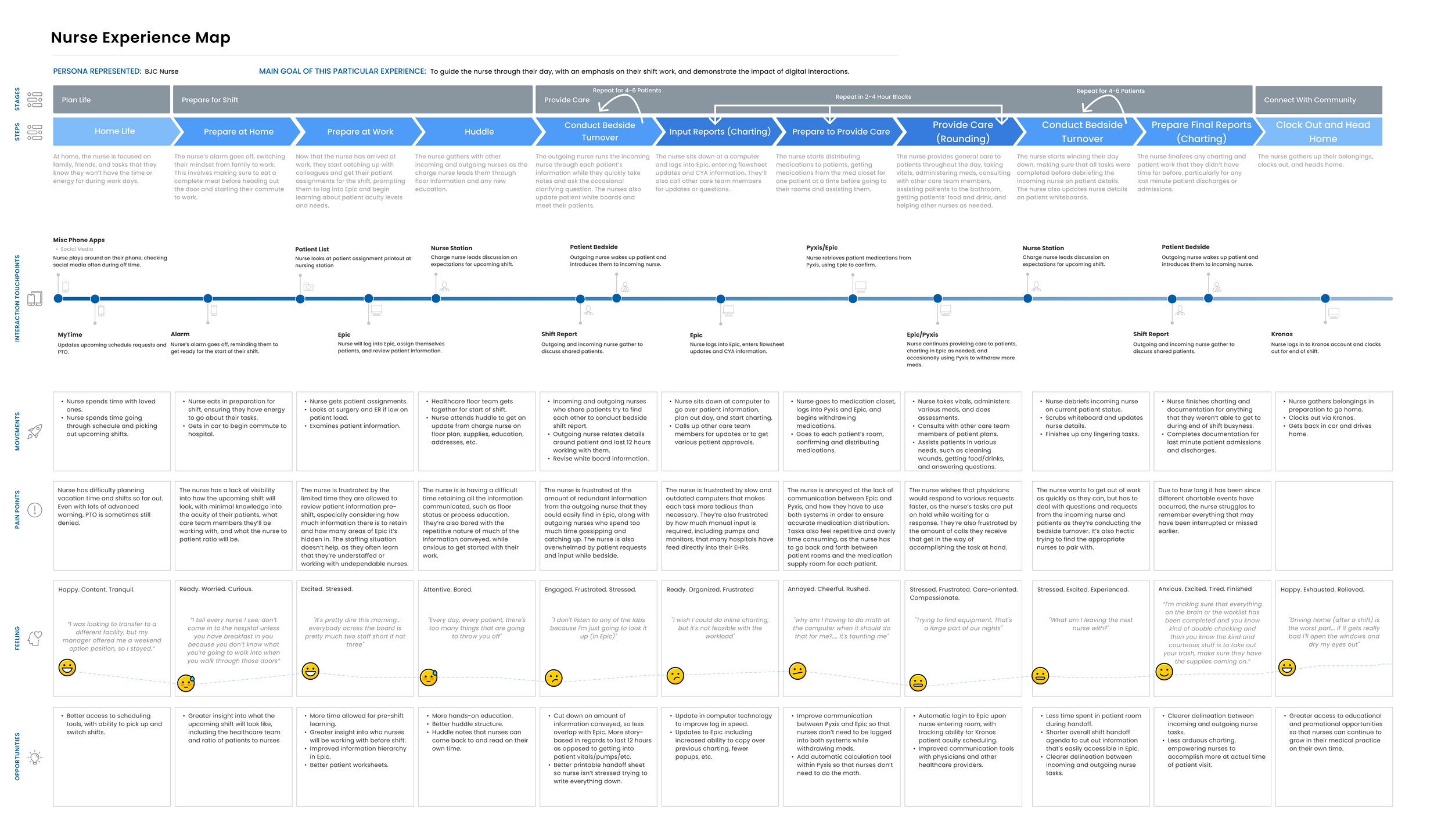
Journey Maps: In an attempt to capture the holistic nurse experience, we broke their journey down into 4 different stages, each with different steps containing their own emotions, pain points, and opportunities; these were Planning Life, Preparing for Shift, Providing Care, and Connecting With Community; each with their own pains, joys, touchpoints, and opportunities.
Personas: While some personas already existed upon my arrival at BJC, these had all either been created before or during the height of the Covid pandemic, when hospital resources were stretched thinnest and nurses at their most burned out. Due to this, we felt the need to update all relevant personas, along with creating completely new personas for roles that had been previously underrepresented and understudied, such as Patient Care Techs.
Outcome & Opportunity
After reviewing the research we concluded that there was a lack of opportunity with the nurse shift hand-off, as, while time-consuming, nurses were shown to mostly enjoy the current process. Nurses found the shift hand-off to be an opportunity to get credit for the work they had performed over the last 12 hours, along with the handwriting process being a good memorization technique for nurses, allowing them to take in and retain more patient information than might be enabled through a digital solution.
However, we were sure to cast a broad net in our research and uncovered other various other potential opportunities, including pump integration, greater electronic health record personalization, improved nurse recognition, and a tool to provide more information about upcoming shifts.
We broke down these opportunities by perceived impact on nurses, likelihood of adoption, and ease of implementation, creating an opportunity matrix that would become our guiding light as we continued moving forward. Out of this, we decided that flexible scheduling, empowering nurses to pick up shifts outside of the typically mandated 12-hour shifts, was the area of greatest opportunity.
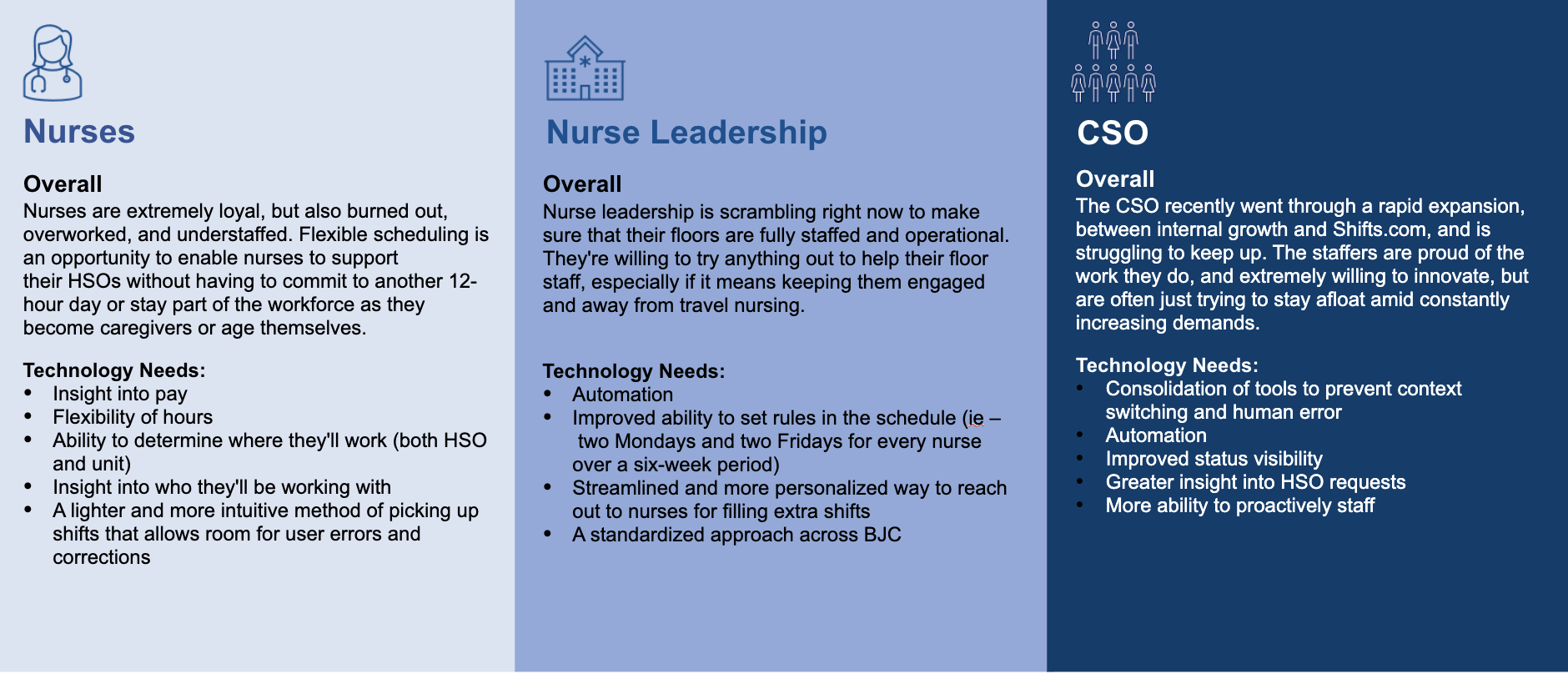
Need Breakdown: Wanting to make sure that all areas were accounted for and that we didn’t focus on only one area of the BJC ecosystem, we broke down the needs, both human and technological, of different layers of the organization, from Floor Nurses, to Nurse Leadership, to the Central Staffing Office (or CSO). This allowed us an easy visual to refer back to while trying to resolve the flexible scheduling dilemma.
Diverging Options
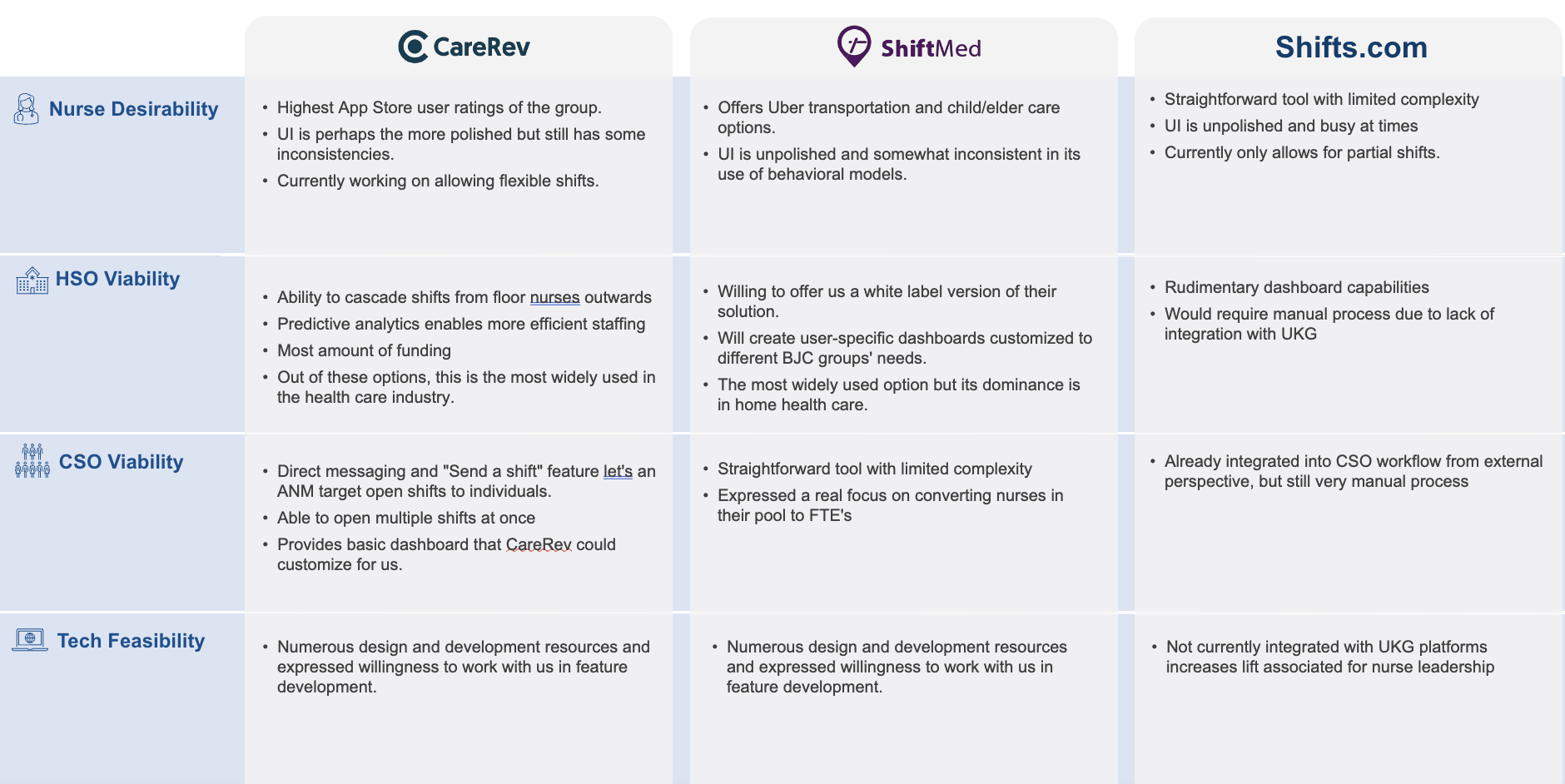
As we started looking at next steps, we had to decide if we wanted to go with an in-house or vended solution to solve the flexible scheduling issue, weighing each option and conducting a competitive analysis of the current environment, landing on CareRev, ShiftMed, and Shifts.com as being the major players in the game at the time.
We also looked at the current technological environment and solution space at BJC, with a solution called Vocantas being the main option for nurses to pick up extra shifts at the time. However, the process was tedious for nurse managers and resulted in notification fatigue for floor nurses, leading to overall low adoption rates.
In-House
Pros:
Flexibility in how we approached the issue and pivoted as needs arose.
We would be able to customize the tool to specifically appeal to BJC nurses.
Cons:
BJC had never created an in-house digital solution.
Uncertainty on process and integrations due to the lack of previous endeavors.
Our team was new and unproven, limiting organizational confidence and buy-in.
Vended Solution
Pros:
There were plenty of quick and easy solutions available to chose from.
Many of the vended solutions had proven track records and a history of success across the country.
Cons:
The vended solutions were often expensive.
Lack of customization due to us being just one client among many.
Many of the vended solutions displayed poor heuristics and UX.
MVP Launch
Once we had gone through the extensive discovery process and research synthesis, we decided that the best course of action was to quickly develop a minimal viable product (MVP) to test the nurse desire and usage for a tool that allowed for a more convenient shift pickup methodology. While we were still debating going the vended solution route, we knew that could take a while due to integration and security concerns, so a quick and dirty pilot could continue keeping us informed in the meantime, and thus what would become known as BJC Flex was born.
Aggressive Time Frame
We gave ourselves 6 weeks to launch a MVP, including design and development, to gauge overall need for a scheduling tool.
The Basics
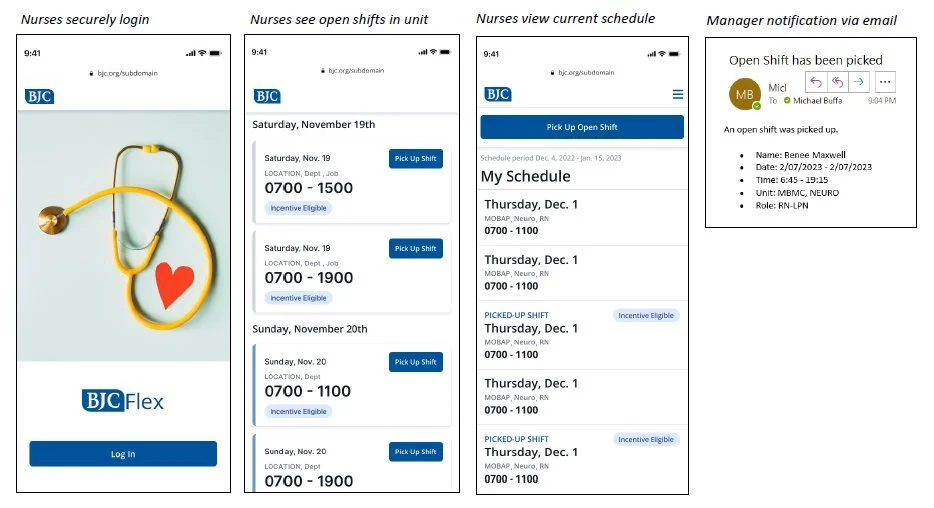
Based off of our previous research and discussions with nurses and nurse managers, we decided that to be successful, any MVP needed to include the ability to:
Ability to have a user login.
Connect to central scheduling software, MyTime.
Display available shifts that individual users were credentialed for.
Allow users to directly pick up shifts and have them be recorded in MyTime.
Accurately display users’ existing schedules.
Notify nurse managers that a shift had been picked up within their unit.
Launch
BJC Flex was initially piloted in two separate units at Missouri Baptist and Christian Hospitals, each with very different staffing levels and needs, to resounding approval. As word spread and adoption rates increased, demand for the new scheduling tool started echoing throughout BJC, leading us to forego the vended solutions, and quickly roll out BJC Flex across our two pilot hospitals before going system-wide, continuing to use adoption rates, feedback, and research to inform our iterative improvements.
In an ecosystem where shifts had been previously picked up in disparate ways, from sheets of paper on manager doors, to verbal requests, to manager calls, having a straightforward and standardized method to pick up shifts was immensely appealing for both nurses and nurse managers. Along with that, nurses loved the ability to conveniently pick up shifts on their own time, picking up additional shifts whenever their floor was in need or they wanted extra cash.
Continued Innovation
Flexible Scheduling: The original impetus behind BJC Flex, this enabled nurses to pick up shifts in increments smaller than the typically mandated 12-hour shift, helping provide greater flexibility and less burnout.
Filtering: The ability to filter what shifts are shown based off of different criteria such as length and unit was one of the most highly requested features from the beginning and was one of our first releases post-MVP.
Calendar View: Another highly requested feature, this allowed nurses to quickly jump to the desired date of a shift pick-up instead of needing to manually scroll. We enhanced this feature later on to indicate when nurses were already working and what days had shifts available based off of their selected filters.
Enhanced Desktop Experience: Research indicated that nurses regularly accessed BJC Flex from desktops, including 16-21% at nurse stations, leading us to optimize the experience for larger screens.
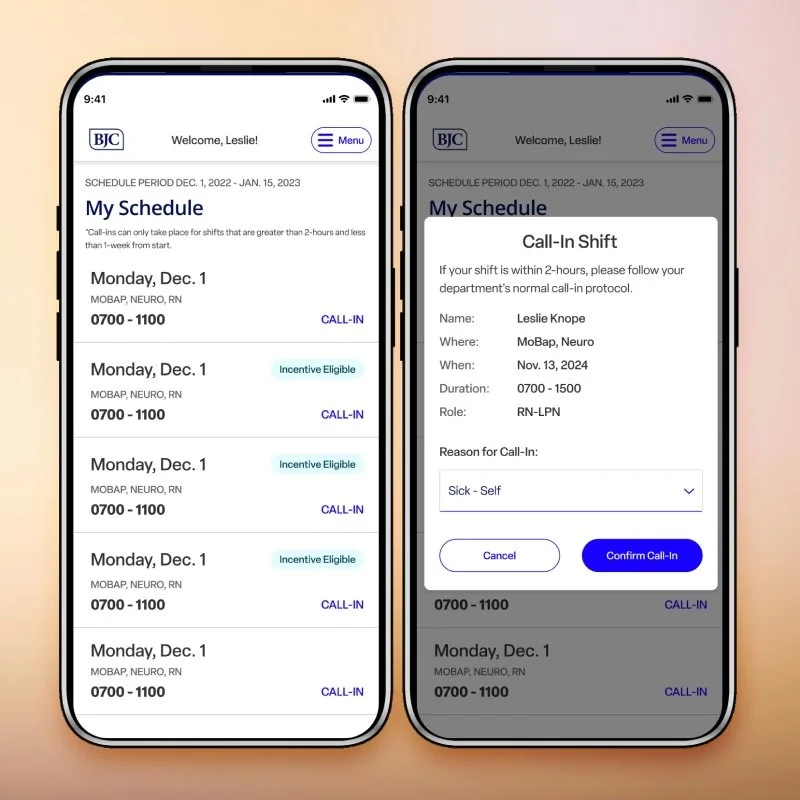
Call-Ins: Digitizing the call-in process, when staff alert management that they won’t be able to make it to a scheduled shift, reduced the need for managers to stop what they were doing to answer the phone for call-ins and automated the reposting of that canceled shift back into BJC Flex.
Results and Impact
Organization
Within the first year of BJC Flex, costly travel nurse usage was reduced by 34%, saving millions of dollars a year.
Less than a year and a half after the pilot was introduced, there had been over 1.4 million shift hours picked up, with an average of 100k+ getting picked up every month.
Standardization across the BJC system empowered nurses to pick up shifts in other units and allowed management to have greater oversight.
Floor Staff
Less reliance on travel nurses allowed for more consistent staffing, increasing trust between staff members and overall satisfaction, along with reducing turnover.
Management
Nurse managers spent an average of 9 hours a week less on manual scheduling and trying to fill shifts, giving them time back to focus on other tasks, improving overall morale and efficiency.
Shift hours picked up as of July 3, 2024, less than a year and a half after the initial pilot launch in two units.